Transarterial Radioembolization (TARE) for Liver Cancer: Treatment for large and advanced liver tumors
If you or someone you love has been diagnosed with a liver tumor, you may have been presented with options like major surgery, systemic chemotherapy, or “watch and wait.” But for many patients, there is another path a targeted, minimally invasive treatment called Transarterial Radioembolization (TARE), also known as Y90 radioembolization.
Liver cancer whether it starts in the liver or spreads there from elsewhere in the body can be difficult to treat because the liver is also essential for digestion, detoxification, and survival. Removing too much liver tissue isn’t always possible. TARE offers a way to attack tumors aggressively while preserving healthy liver function. This guide explains everything patients and caregivers need to know about TARE.
Understanding Liver Tumors: Why TARE Is Used
The liver is the body’s largest internal organ, responsible for filtering toxins, producing bile, and regulating metabolism. Tumors in the liver generally fall into two categories:
Primary liver cancer: cancer that originates in the liver itself, most commonly hepatocellular carcinoma (HCC), often linked to chronic hepatitis B/C infection, cirrhosis, or fatty liver disease.
Metastatic (secondary) liver tumors : cancer that has spread to the liver from another organ, most often the colon, breast, pancreas, or lung.
Common Symptoms
Many liver tumors are silent in their early stages and are found incidentally during imaging for another condition. As they grow, symptoms may include:
- Upper right abdominal pain or fullness
- Unexplained weight loss
- Fatigue and weakness
- Loss of appetite
- Yellowing of the skin or eyes (jaundice)
- Swelling in the abdomen (ascites)
How Liver Tumors Are Diagnosed
Diagnosis typically involves blood tests (including tumor markers like AFP), imaging such as ultrasound, CT, or MRI, and sometimes a biopsy. Staging the tumor its size, number, and how well the liver is functioning determines which treatments are appropriate.
Traditional Liver Cancer Treatments and Their Limitations
Liver tumor management has traditionally relied on a few main approaches, each with real trade-offs.
- Surgical Resection: Removing the tumor along with a margin of healthy liver tissue can be curative, but it’s only an option when the tumor is small, well-located, and the remaining liver can still function adequately. Many patients aren’t eligible due to tumor size, number, location, or poor underlying liver health.
- Liver Transplantation: An option for select early-stage HCC patients, but limited by donor organ availability, long waiting times, and the need for lifelong immunosuppression.
- Systemic Chemotherapy and Targeted/Immunotherapy: Effective for controlling disease throughout the body, but it affects healthy tissue along with cancerous tissue and often comes with significant side effects like fatigue, nausea, and immune suppression.
- Transarterial Chemoembolization (TACE) Similar in concept to TARE, but delivers chemotherapy drugs (instead of radiation) directly into the tumor’s blood supply. It’s widely used but generally requires repeat sessions and can cause more post-procedure pain and inflammation than TARE.
- Thermal Ablation (Radiofrequency/Microwave Ablation): Effective for small, solitary tumors, but less suitable for larger tumors or those located near major blood vessels or other organs.
These limitations are part of why interventional radiologists increasingly turn to TARE — particularly for patients who aren’t candidates for surgery, have larger or multiple tumors, or need a treatment that can be combined with other therapies.
What Is TARE and How Does It Work?
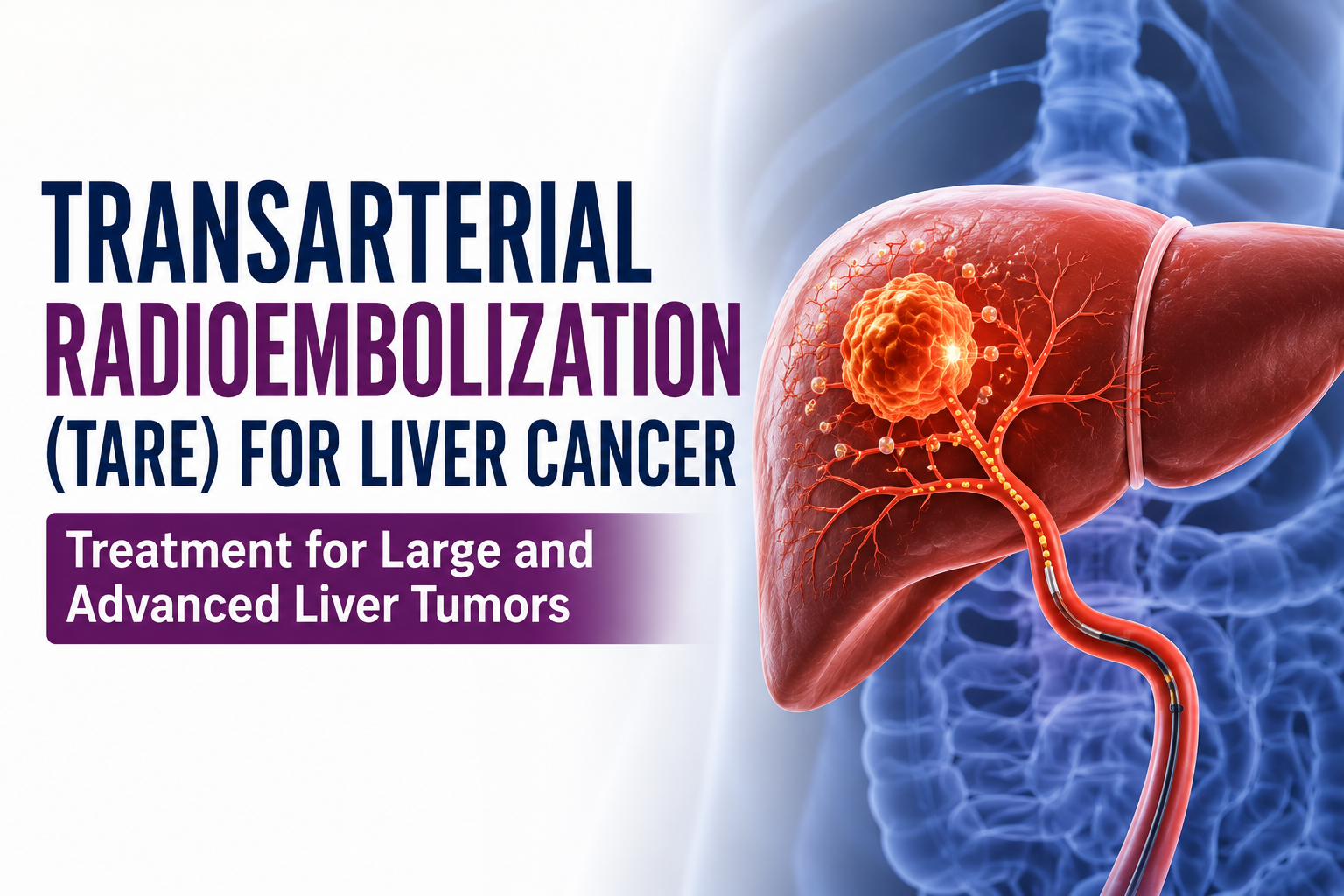
Transarterial Radioembolization is a minimally invasive, image-guided procedure performed by an interventional radiologist. Instead of cutting out the tumor or delivering radiation from outside the body, TARE delivers radiation from the inside directly into the blood vessels feeding the tumor.
The “active ingredient” is Yttrium-90 (Y90), a radioactive isotope embedded in microscopic beads called microspheres, roughly the width of a few human hairs. Because liver tumors typically draw their blood supply almost entirely from the hepatic artery (while healthy liver tissue relies more on the portal vein), these microspheres can be delivered in a way that concentrates radiation in the tumor while relatively sparing surrounding healthy liver.
Once injected, the microspheres lodge in the small vessels around the tumor and emit radiation over the following days to weeks, damaging cancer cells from within.
What Outcomes Can TARE Achieve?
TARE is used both to shrink or control tumors directly and, in some cases, to shrink a tumor enough that surgery or transplantation becomes possible. For patients with unresectable HCC or liver-dominant metastatic disease, TARE has been shown in clinical studies to achieve meaningful local tumor control and disease stabilization, with the specific benefit varying based on tumor type, size, liver function, and overall health. Your oncology and interventional radiology team will discuss what outcome is realistic for your specific case.
Who Is a Candidate for TARE?
TARE isn’t a one-size-fits-all treatment, but it’s an excellent option for a carefully selected group of patients.
You may be a good candidate if you have:
- Primary liver cancer (HCC) not suitable for surgery or transplant
- Liver metastases from colorectal, breast, or other cancers, largely confined to the liver
- Tumors too large or numerous for ablation alone
- Adequate liver function despite the tumor burden
- A need for tumor downstaging before surgery or transplant
- A preference to avoid major surgery or its recovery time
TARE may not be suitable if you have:
- Significant liver dysfunction or advanced cirrhosis
- Tumor blocking major blood flow to the liver in certain patterns
- Widespread cancer outside the liver with poor overall prognosis
- Inability to tolerate the angiography procedure
- Certain lung shunting patterns identified during pre-treatment mapping
The TARE Procedure: Step by Step
- Pre-Procedure Mapping (Work-up Angiogram): Before treatment, the interventional radiologist performs a mapping angiogram and injects a small test dose to check blood flow patterns and rule out unsafe shunting to the lungs or stomach. Imaging and blood tests confirm candidacy.
- Catheter Access: Under local anesthesia and light sedation, a thin catheter is inserted through an artery in the wrist or groin and guided, using live imaging, into the hepatic artery branches feeding the tumor.
- Treatment Planning: Based on the mapping results, the team calculates a precise, personalized dose of Y90 microspheres.
- Radioembolization: During the treatment session (usually scheduled one to two weeks after mapping), the Y90 microspheres are slowly injected into the targeted vessels.
- Recovery and Monitoring: The catheter is removed, and patients are monitored for a few hours. Most go home the same day or after a short overnight stay.
Procedure Duration: The treatment session itself typically takes 60–90 minutes, not including pre-procedure preparation.
Benefits of TARE
- No large incisions or general anesthesia in most cases
- Outpatient or short overnight stay
- Targeted radiation delivery that spares much of the healthy liver
- Can treat larger or multiple tumors that aren’t suitable for ablation
- May be combined with other treatments (surgery, systemic therapy, transplant)
- Generally well tolerated, with fewer post-procedure symptoms than TACE
- Can be repeated or adjusted if needed
Potential Risks and Side Effects
TARE is generally safe when performed by an experienced interventional radiology team, though, like any medical procedure, it carries some risk.
Common Temporary Side Effects
- Fatigue, sometimes lasting one to two weeks (“post-radioembolization syndrome”)
- Mild abdominal discomfort or nausea
- Low-grade fever
- Loss of appetite for a few days
Less Common Risks
- Changes in liver function tests requiring monitoring
- Bruising or discomfort at the catheter access site
- Gastric or duodenal irritation if microspheres reach nearby vessels
Rare Serious Complications
- Radiation-induced liver disease
- Non-target embolization affecting nearby organs
- Lung inflammation related to shunting (screened for during mapping)
Major complication rates are low when proper pre-procedure mapping and dosimetry are followed.
Conclusion
Transarterial Radioembolization offers a targeted, minimally invasive way to fight liver tumors while helping preserve quality of life and healthy liver function. For patients who aren’t candidates for surgery or who want to avoid it TARE can be a valuable part of the treatment plan, often used alongside surgery, systemic therapy, or transplantation. If you’ve been diagnosed with a liver tumor, consult our best interventional radiologist whether TARE could be right for you.
FAQs:
Is TARE painful?
Most patients experience only mild discomfort at the catheter site and some fatigue in the days following the procedure. General anesthesia is usually not required.
How is TARE different from TACE?
TACE delivers chemotherapy drugs to the tumor’s blood supply, while TARE delivers targeted radiation via Y90 microspheres. TARE is often better tolerated, with less post-procedure pain and inflammation.
How many TARE sessions are needed?
Many patients are treated in one or two sessions, though this depends on tumor size, number, and location in each liver lobe.
Will TARE cure my cancer?
TARE can control or shrink tumors and, in some cases, help downstage disease for surgery or transplant. Whether it offers a cure depends heavily on the type and stage of cancer your care team can explain what to expect in your specific case