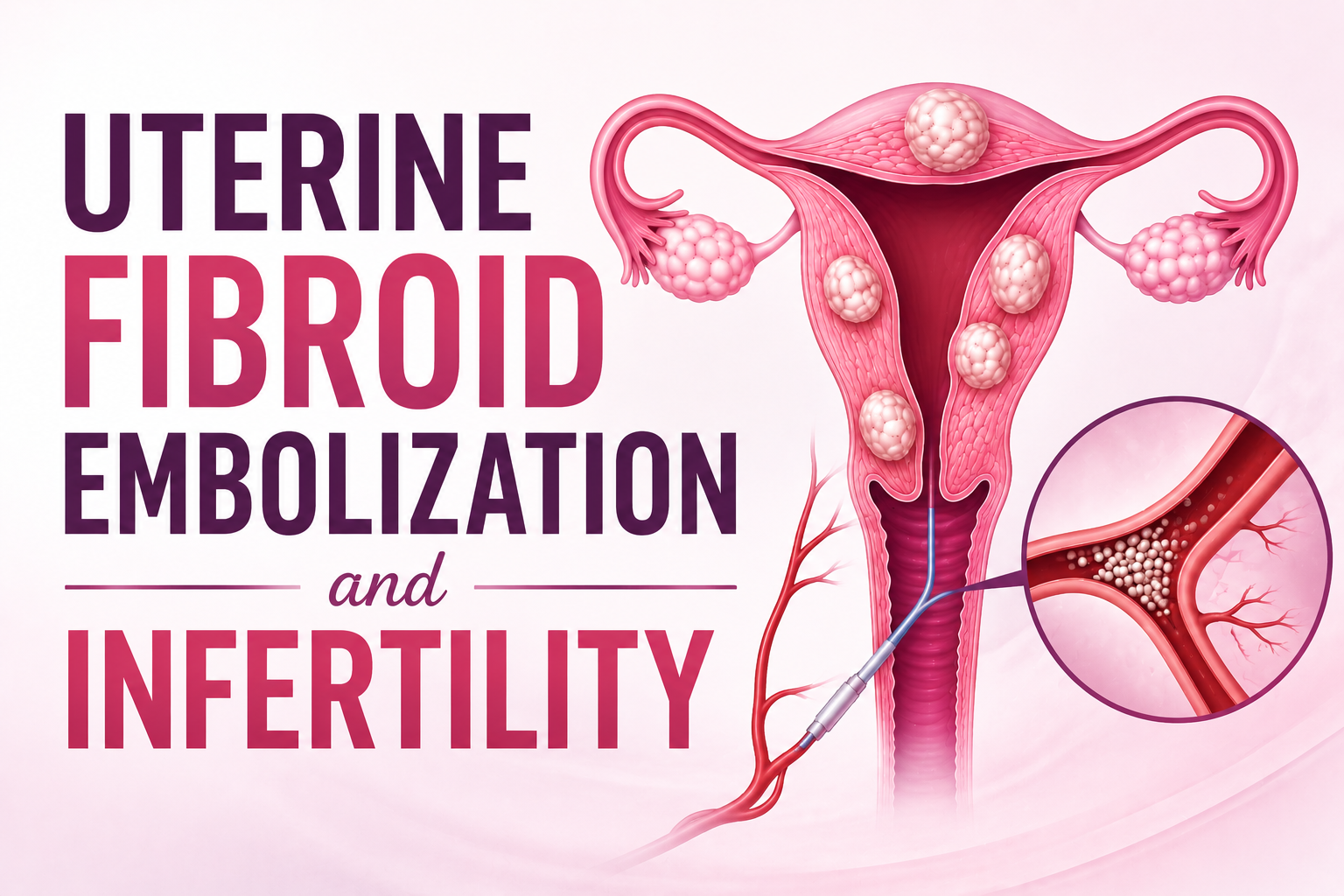
Uterine Fibroid Embolization and Infertility
Uterine fibroids affect a large number of women during their reproductive years, and for many they raise a difficult question: can the fibroids be treated effectively without putting future fertility at risk? It is one of the most common concerns women have when they first learn that treatment is needed.
The answer depends a great deal on the type of treatment chosen and on a woman’s own reproductive plans. Interventional Radiology now offers minimally invasive, uterus-preserving options chiefly Uterine Fibroid Embolization (UFE) and Microwave Ablation (MWA) that treat fibroids without major surgery. Understanding how each works, and where each fits, helps women make a confident, informed decision.
Understanding Uterine Fibroids
Uterine fibroids, medically known as leiomyomas, are non-cancerous growths that form in or around the uterus. They differ widely in size, number, and position, and are usually grouped by location
- Submucosal fibroids – project into the cavity of the uterus
- Intramural fibroids – sit within the muscular wall
- Subserosal fibroids – grow on the outer surface
Many women have fibroids without ever knowing it. When symptoms do occur, they commonly include heavy or prolonged menstrual bleeding, pelvic pain or pressure, frequent urination, constipation, discomfort during intercourse, and in some cases difficulty conceiving or repeated miscarriage.
How Fibroids Can Affect Fertility
Fibroids do not always interfere with fertility, and many women conceive without difficulty. However, depending on their size and position, some fibroids can reduce the chances of pregnancy by distorting the uterine cavity, obstructing the fallopian tubes, interfering with embryo implantation, limiting blood flow to the uterine lining, or raising the risk of miscarriage.
Submucosal fibroids and large intramural fibroids are most often linked to these problems, because they directly affect the shape and function of the uterus. This is why any decision about treatment must take a woman’s fertility goals into account, not just the appearance of the fibroids on a scan.
Minimally Invasive Treatments in Interventional Radiology
Microwave Ablation (MWA)
Microwave Ablation is a targeted, image-guided technique. A fine probe is placed directly into a fibroid, and microwave energy produces heat that destroys the fibroid tissue while leaving the surrounding healthy uterine tissue intact.
Because it focuses on individual fibroids with precision, MWA is sometimes considered for selected younger women, including some who may wish to conceive in the future. Current studies show it can reduce fibroid size, ease symptoms, improve quality of life, and help correct anaemia. It is worth noting, however, that detailed evidence on pregnancy outcomes specifically after fibroid microwave ablation is still limited, so it is best viewed as a carefully selected option rather than an established fertility treatment.
Reported benefits of MWA include precise treatment of selected fibroids, preservation of the uterus, minimal blood loss, a short hospital stay, and a quick recovery.
Uterine Fibroid Embolization (UFE)
Uterine Fibroid Embolization treatment in Hyderabad works differently. Rather than treating each fibroid individually, it cuts off the blood supply that feeds them. Through a small puncture in the wrist or groin — without any surgical incision — a thin catheter is guided to the uterine arteries, and tiny particles are released to block the flow of blood to the fibroids. Deprived of their blood supply, the fibroids gradually shrink, and symptoms ease over the weeks and months that follow.
The main advantage of UFE is its ability to treat every fibroid in the uterus in a single procedure, no matter how many are present. It is also the most established and extensively studied minimally invasive fibroid treatment, supported by decades of clinical experience.
Reported benefits of UFE include effective treatment of multiple fibroids at once, preservation of the uterus, no major incision, a short hospital stay, reduced blood loss, a faster recovery than surgery, and durable, long-term symptom relief.
UFE and Fertility: An Honest Perspective
A common misconception is that UFE inevitably causes infertility. The reality is more nuanced. Pregnancies have certainly occurred after UFE, and in some women the shrinking of fibroids can improve the shape of the uterine cavity. At the same time, the overall evidence on fertility after UFE is mixed, and some studies have suggested a slightly higher risk of miscarriage.
For this reason, UFE is generally not regarded as the first-choice treatment for women who are actively trying to conceive. In those cases, surgical removal of the fibroids (myomectomy) has long been the preferred fertility-preserving approach, as it has the clearest evidence base for subsequent pregnancy.
Where UFE truly stands out is in a different group of women.
Why UFE Is Well Suited to Women Who Have Completed Their Family
For women who have completed their family or who are not planning a pregnancy UFE is one of the most effective and convenient treatments available. The mixed fertility evidence becomes far less relevant, while all of UFE’s strengths come to the fore:
- Reliable, lasting relief from heavy bleeding, pain and pressure
- Treatment of multiple fibroids in a single procedure
- Preservation of the uterus, avoiding hysterectomy
- A quick recovery, with most women resuming normal activities within days
- The strongest long-term track record of any minimally invasive fibroid treatment
- Freedom from the risks of open surgery and general anaesthesia
For these women, UFE offers durable symptom control without major surgery, making it an excellent and well-evidenced choice.
Choosing Between MWA and UFE
Neither treatment is universally “better” they serve different needs:
- MWA is generally considered when there are one or a few well-defined fibroids in accessible locations, where targeted treatment is appropriate, and occasionally for selected younger patients, with clear counselling about the limits of current fertility evidence.
- UFE is generally preferred when there are multiple fibroids or widespread symptoms, and especially for women who have completed their family and want the most established, long-proven option.
The right choice depends on the number, size, and location of the fibroids, the severity of symptoms, and most importantly the woman’s pregnancy plans. A personalised assessment ideally involving an interventional radiologist helps identify the best path.
Who Is a Good Candidate?
Minimally invasive fibroid treatment may be appropriate for women who:
- Experience heavy menstrual bleeding, pelvic pain, or pressure
- Have multiple fibroids they would prefer not to remove surgically
- Wish to preserve the uterus
- Have completed their family and want long-term symptom relief
- Prefer to avoid major surgery and a lengthy recovery
- Are not ideal candidates for surgery
Women considering a future pregnancy should undergo a thorough fertility evaluation before choosing any treatment.
Recovery
Recovery after both procedures is generally quick. Following UFE, mild cramping for a day or two is common as the fibroids begin to shrink, and is easily managed with pain relief; most women return to normal activity within a few days. Recovery after MWA is similar. In both cases, periods typically become lighter and pelvic pressure eases over the following months, with energy improving as anaemia resolves. Follow-up confirms that the fibroids are shrinking as expected.
Frequently Asked Questions
Does uterine fibroid embolization cause infertility? UFE does not automatically cause infertility, and pregnancies have occurred afterwards. However, the evidence on fertility after UFE is mixed, which is why it is not usually the first choice for women actively planning a pregnancy.
Which treatment is best for women who have completed their family?
UFE is particularly well suited to this group. It provides effective, lasting relief from fibroid symptoms while preserving the uterus and avoiding major surgery, and it has the strongest long-term evidence of any minimally invasive option.
Is microwave ablation a fertility-preserving treatment?
MWA preserves the uterus and may be considered for selected women hoping to conceive, but specific pregnancy data after fibroid MWA remains limited. It should be discussed carefully on a case-by-case basis.
What is the preferred treatment if pregnancy is the goal?
Myomectomy — surgical removal of the fibroids — is generally the preferred fertility-preserving option, as it has the clearest evidence for subsequent pregnancy.
Can fibroids return after treatment?
Treated fibroids usually shrink and do not regrow, though new fibroids can develop over time in some women, occasionally requiring further treatment.
How long should a woman wait before trying to conceive?
Most specialists recommend waiting roughly six months to allow the fibroids to shrink and the uterus to heal, and advise planning treatment with fertility goals in mind from the start.
Conclusion
Fibroid treatment is most successful when it is matched to a woman’s individual symptoms and reproductive goals. For those planning a pregnancy, fertility-preserving options such as myomectomy, and in selected cases microwave ablation, deserve careful consideration. For women who have completed their family and are seeking a minimally invasive alternative to surgery, Uterine Fibroid Embolization stands out offering proven, durable relief, treatment of multiple fibroids at once, and preservation of the uterus. Any woman troubled by fibroid symptoms can benefit from a consultation with our best interventional radiologist, who can help determine the most suitable treatment for her individual needs.
About the Author:

Name: DR . SURESH GIRAGANI
INTERVENTIONAL RADIOLOGIST
DR. SURESH GIRAGANI CONSULTANT INTERVENTIONAL RADIOLOGIST at Apollo hospitals Jubilee Hills has more than Seventeen years of clinical experience in vascular interventions with a special interest in neurovascular and peripheral vascular disease interventional procedures.