Cryoablation for Abdominal Tumors
For decades, surgery was the default answer whenever a tumor was found in the abdomen. Open or laparoscopic resection meant general anesthesia, days of hospital recovery, and meaningful risk for patients who were older, frail, or living with other health conditions. Cryoablation has changed that equation. By guiding a thin probe directly into a tumor and freezing it to lethal temperatures, interventional radiologists can now destroy many abdominal tumors through a single small skin puncture, often as an outpatient or overnight procedure.
This blog explains what cryoablation is, how it works inside the abdomen specifically, which tumors respond best, what patients can expect before and after the procedure, and how it compares with surgery and other ablation techniques.
What Is Cryoablation?
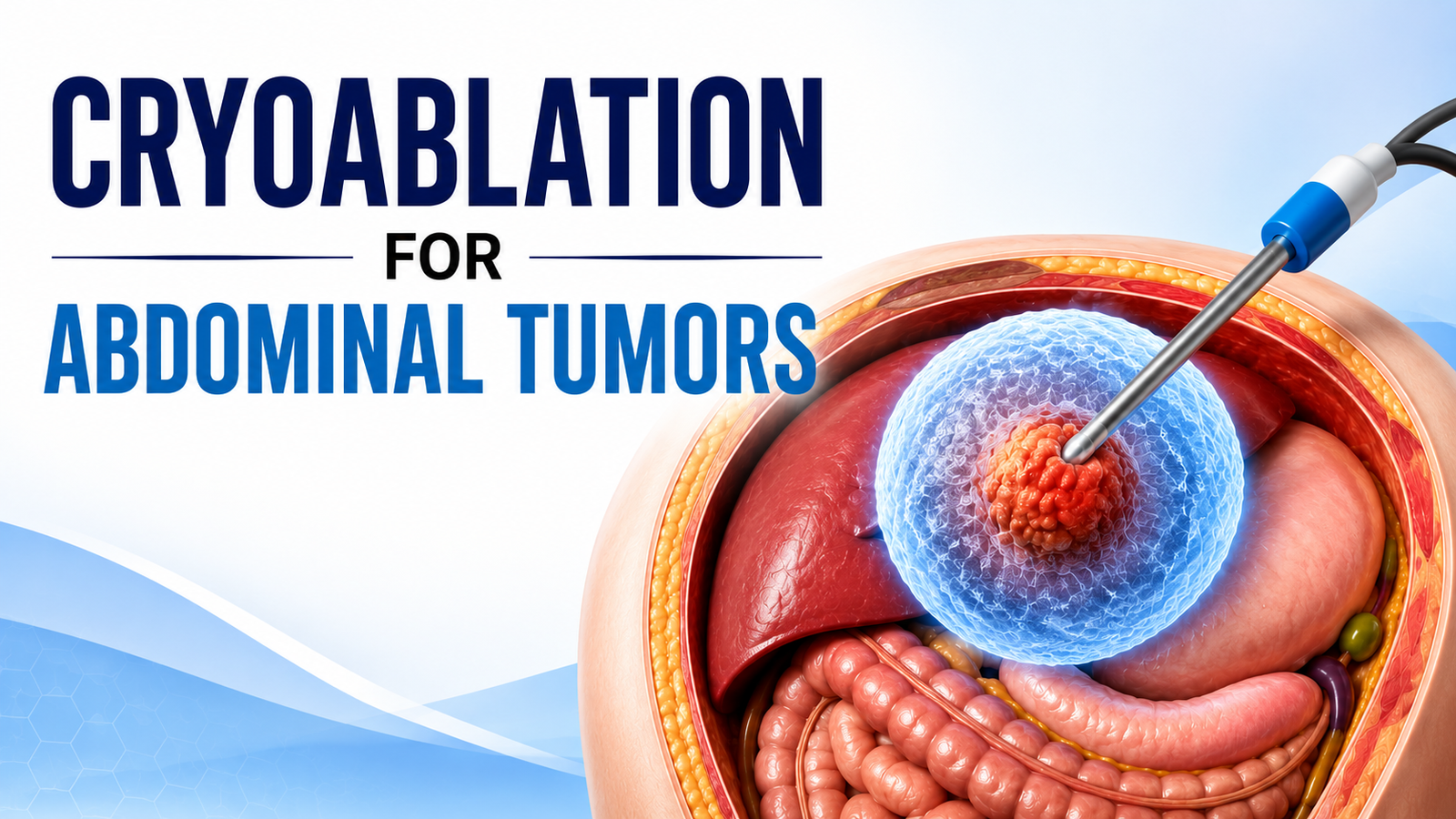
Cryoablation, sometimes called cryotherapy or cryosurgery, is a form of image-guided tumor destruction that uses extreme cold instead of heat, radiation, or chemotherapy. A radiologist inserts one or more hollow, needle-thin cryoprobes through the skin and into the tumor using CT, MRI, or ultrasound guidance. Pressurized argon gas circulating inside the probe tip causes a rapid temperature drop through the Joule-Thomson effect, and the tip can reach roughly -100°C to -150°C within minutes.
As the probe cools, a visible ball of ice forms around the tip and grows outward to encompass the tumor along with a safety margin of surrounding tissue. The freeze-thaw cycle is typically repeated twice, since cell death is more complete on the second cycle. Ice crystals form inside and around tumor cells, rupturing cell membranes, disrupting blood flow to the area, and triggering the cell death that ultimately destroys the lesion.
Why Freezing Instead of Heat?
Heat-based ablation methods such as radiofrequency or microwave ablation are also widely used in the abdomen, but cryoablation has a few distinct advantages that make it especially useful for certain locations and patient types:
Visible margins: The ice ball is clearly visible on CT and MRI in real time, letting the physician confirm that the entire tumor and only the tumor is being treated.
Less pain: Many patients report less procedural and post-procedural pain with freezing compared to heat-based methods, possibly because cold has a numbing effect on nerve tissue.
Multi-probe flexibility: Multiple probes can be placed simultaneously and arranged around a tumor of unusual shape, which is useful for larger or irregular masses.
Vessel-friendly profile: Cryoablation carries a lower risk of damaging large blood vessels because frozen tissue near vessels is somewhat protected by the warming effect of flowing blood, a phenomenon known as the heat-sink effect though this same effect can occasionally make tumors near big vessels harder to fully ablate.
Which Abdominal Tumors Can Be Treated with Cryoablation?
Cryoablation is most established and best studied for small kidney tumors, but its use has expanded to several other abdominal organs as devices, imaging guidance, and operator experience have matured.
Kidney (Renal) Tumors
Small renal masses, generally those under 3 to 4 cm, are the most common indication for abdominal cryoablation. It is particularly suited to patients who are poor surgical candidates due to age, reduced kidney function, multiple medical problems, or tumors in both kidneys. Because cryoablation preserves healthy surrounding kidney tissue, it is considered a nephron-sparing option, similar in philosophy to partial nephrectomy but without open or laparoscopic surgery.
Liver Tumors
Cryoablation can treat both primary liver cancer (hepatocellular carcinoma) and metastases that have spread to the liver from cancers such as colorectal cancer. It is especially considered for tumors located near the liver capsule, diaphragm, gallbladder, or major vessels, sites where heat-based ablation can sometimes under-treat the lesion or risk thermal injury to adjacent structures.
Adrenal Gland Tumors
Adrenal tumors, including some metastatic lesions, can be treated with percutaneous cryoablation when surgery carries elevated risk. Careful blood pressure monitoring is required during treatment of certain adrenal lesions because of the gland’s hormone-producing tissue.
Pancreatic Tumors
Pancreatic applications are more limited and typically reserved for select cases, often in combination with other treatments, given the pancreas’s sensitivity and proximity to major vessels and the bowel.
Desmoid tumor:
Desmoid tumors (desmoid-type fibromatosis) are benign but locally aggressive soft tissue tumors that often recur after surgery, with recurrence rates reported up to 60%. Repeated surgeries can be challenging and increase the risk of damage to nearby nerves, blood vessels, and organs. As a result, cryoablation has emerged as an effective minimally invasive treatment for recurrent, unresectable, or medication-resistant desmoid tumors. It provides excellent local tumor control, with reported progression-free survival of about 89% at one year, while also reducing pain and improving mobility. Since the procedure can be repeated if the tumor returns, cryoablation is particularly well suited for managing this recurrence-prone condition.
Other Abdominal and Retroperitoneal Sites
Selected soft tissue tumors, certain metastatic deposits, and recurrences in the abdominal wall or retroperitoneum may also be candidates depending on size, location, and proximity to bowel or major vessels.
What Happens During the Procedure?
Most abdominal cryoablation procedures follow a similar sequence, though exact details vary by hospital and tumor location.
Pre-procedure imaging and planning: CT, MRI, or PET scans are reviewed to map the tumor’s exact size, shape, and relationship to nearby organs and vessels.
Anesthesia: The procedure is usually done under conscious sedation or general anesthesia, depending on tumor location and patient factors.
Probe placement: Using real-time CT, MRI, or ultrasound guidance, the radiologist inserts one or more cryoprobes directly into the tumor through a small skin nick, no larger than a few millimeters.
Freezing: Argon gas cools the probe tips, forming a visible ice ball that engulfs the tumor with a margin of healthy tissue. Two freeze-thaw cycles are typically performed.
Thaw and probe removal: Helium gas or a warming cycle thaws the probe so it can be safely removed; a small dressing is applied to the skin entry site.
Recovery: Patients are observed for several hours and most go home the same day or after one overnight stay.
Recovery and Follow-Up
Most patients resume light daily activities within a few days. Mild soreness, low-grade fever, or temporary changes in urine color (for kidney procedures) are common in the first 48 hours and typically resolve on their own. Follow-up imaging, usually at one, three, six, and twelve months, confirms the ablated tissue has scarred down without signs of residual or recurrent tumor.
Benefits and Risks
Potential Benefits
Minimally invasive: No large incision, general anesthesia is often avoidable, and most patients return home the same day or after one night.
Organ-sparing: Cryoablation preserves more healthy tissue than surgical resection, which matters most for organs like the kidney.
Lower systemic burden: Suitable for patients who cannot safely undergo general anesthesia or major surgery.
Repeatable: Procedures can often be repeated if new tumors develop or if a treated area shows incomplete response.
Potential Risks
- Bruising, mild pain, or fluid collection at the treatment site.
- Bleeding, infection, or injury to nearby structures such as bowel, ureter, or major vessels, though these are uncommon with image guidance.
- Incomplete ablation, particularly with larger tumors or those near major vessels, which can require repeat treatment.
- Cryoshock phenomenon: Rare but recognized complication when freezing large tumor volumes, most often associated with bigger renal masses.
As with any procedure, the treating physician will weigh these risks against the benefits based on the specific tumor and the patient’s health profile.
Is Cryoablation Right for You?
Cryoablation is not a one-size-fits-all answer, but for the right tumor in the right location, it offers a compelling combination of precision, reduced invasiveness, and faster recovery compared to traditional surgery. The decision is best made by a multidisciplinary team that includes the best interventional radiologist in Hyderabad.
Frequently Asked Questions
Is cryoablation painful?
The procedure itself is performed under conscious sedation or general anesthesia, so patients feel nothing during treatment. Afterward, most experience only mild soreness at the skin entry site for a day or two, which is easily managed with simple pain relief. Many patients actually report less pain with freezing than with heat-based ablation, as cold has a numbing effect on nerve tissue.
How long does recovery take?
Most patients go home the same day or after a single overnight stay and return to light daily activities within a few days, a marked contrast to the weeks of recovery that can follow open surgery.
Is cryoablation as effective as surgery?
For small, well-selected tumors, cryoablation can offer excellent local control while sparing far more healthy tissue. Surgery still has longer-term data for certain cancers, which is why the choice is made tumor by tumor. For specific situations such as small kidney tumors or recurrent desmoid tumors cryoablation is increasingly considered comparable to surgery with lower morbidity.
Why use cryoablation for a recurrent desmoid tumor instead of more surgery?
Desmoid tumors recur after surgery in a high proportion of cases, and each repeat operation becomes more difficult and riskier to surrounding nerves, bowel, and vessels. Cryoablation offers strong local control and significant relief from pain and stiffness without another major operation, and it can be repeated if the tumor regrows making it well suited to such a recurrence-prone condition.
Can cryoablation be repeated?
Yes. One of its practical advantages is that it can be repeated if a new tumor develops or if a treated area shows an incomplete response, without burning bridges to other treatment options.
Will I need to stay in hospital?
In most cases cryoablation is an outpatient or single-overnight procedure, depending on the tumor’s location and the patient’s overall health.
What are the main risks?
Serious complications are uncommon with image guidance. Possible issues include bruising or mild pain at the site, a small risk of bleeding or injury to nearby structures, and incomplete ablation of larger tumors. A rare complication called cryoshock can occur when freezing very large tumor volumes. The treating physician reviews the specific risks for each tumor before the procedure.
About the Author:

Name: DR . SURESH GIRAGANI
INTERVENTIONAL RADIOLOGIST
DR. SURESH GIRAGANI CONSULTANT INTERVENTIONAL RADIOLOGIST at Apollo hospitals Jubilee Hills has more than Seventeen years of clinical experience in vascular interventions with a special interest in neurovascular and peripheral vascular disease interventional procedures.