Types of Flow Diverter Stents & Post-Operative Side Effects

If you or someone you love has been told they have an abnormal enlargement of the thyroid gland you may have been presented with two options: lifelong medication or surgery. But today, there is a third, highly effective, minimally invasive path: Thyroid Artery Embolization (TAE).
Millions of people across the world live with thyroid disorders. Goitre is among the most visible and physically uncomfortable of these conditions. Yet the fear of surgery, the risk of complications, and the prospect of a long recovery often keep patients from seeking timely treatment. This guide explains everything patients and caregivers need to know about Thyroid Artery Embolization for goitre .
What Is a Goitre? Understanding the Condition
The thyroid gland is a small, butterfly-shaped gland sitting at the front of your neck, just below the Adam’s apple. It produces hormones primarily thyroxine (T4) and triiodothyronine (T3) that regulate metabolism, heart rate, body temperature, and energy levels.
A goitre is simply the term for an abnormal enlargement of this gland. It can range from a barely noticeable swelling to a dramatic enlargement that causes visible neck distortion and significant compression of surrounding structures including the windpipe (trachea), food pipe (oesophagus), and blood vessels.
There are several types of goitre:
Diffuse goitre — the entire gland is uniformly enlarged (often associated with Graves’ disease or iodine deficiency)
Nodular goitre — one or more nodules (lumps) develop within the gland
Multinodular goitre (MNG) — multiple nodules, the most common form requiring intervention
Toxic goitre — an overactive (hyperthyroid) gland associated with excess hormone production
Endemic goitre — Endemic goitre caused by iodine deficiency in a specific geographic region
Symptoms and Causes of Goitre:
Common Symptoms
Many small goitres c:ause no symptoms and are often found during routine check-ups or ultrasounds. As the thyroid enlarges, symptoms may include:
- Swelling or fullness in the neck
- Tightness or pressure in the throat
- Difficulty swallowing or breathing
- Hoarseness or voice changes
- Persistent cough or sensation of a lump in the throat
- Dizziness when raising the arms
- Symptoms of thyroid imbalance such as fatigue, weight changes, palpitations, or heat/cold intolerance
What Causes a Goitre?:
Goitre develops when the thyroid gland is stimulated beyond its normal function. The most common causes include:
Iodine deficiency — the most common worldwide cause, especially in landlocked or mountainous regions
Hashimoto’s thyroiditis — an autoimmune disease that attacks the thyroid
Graves’ disease — an autoimmune disorder causing hyperthyroidism and diffuse goitre
Thyroid nodules — Thyroid nodules are benign or rarely malignant growths within the gland
Pregnancy — elevated HCG levels stimulate the thyroid temporarily
Genetic factors — family history of thyroid disease
Medications — lithium, amiodarone, and certain other drugs can cause goitre
Radiation exposure to the head and neck
Traditional Goitre Treatments — and Their Limitations
The management of goitre has traditionally revolved around three pillars:
- Watchful Waiting (Observation)
For small, asymptomatic goitres, a “wait and watch” approach with periodic ultrasound monitoring may be appropriate. However, goitres rarely resolve on their own and often slowly enlarge over months to years.
- Medical Therapy (Thyroid Hormone Suppression)
Thyroxine tablets are sometimes prescribed to suppress TSH and reduce gland stimulation. Results are modest at best — studies show average volume reduction of only 10–20% — and the therapy requires long-term compliance, regular monitoring, and carries risks of bone loss and cardiac effects over time.
- Radioactive Iodine (RAI) Therapy
Radioiodine (I-131) can reduce goitre volume by 30–50% over 12–24 months. However, it is contraindicated during pregnancy and breastfeeding, may worsen thyroid eye disease in Graves’ patients, requires radiation precautions, and carries a significant risk of permanent hypothyroidism requiring lifelong thyroid hormone replacement.
- Thyroid Surgery (Thyroidectomy)
Partial or total surgical removal of the thyroid gland has historically been the gold standard for large, symptomatic goitres
It is effective but carries genuine risks:
Thyroid surgery may involve risks such as anesthesia complications, lifelong thyroid hormone replacement, low calcium levels, voice changes, neck scarring, and a recovery period of several weeks. These risks are higher in elderly patients and those with heart, lung, or other medical conditions, making many poor candidates for surgery — where Thyroid Artery Embolization (TAE) can offer a safer alternative.
- What Is Thyroid Artery Embolization (TAE)?
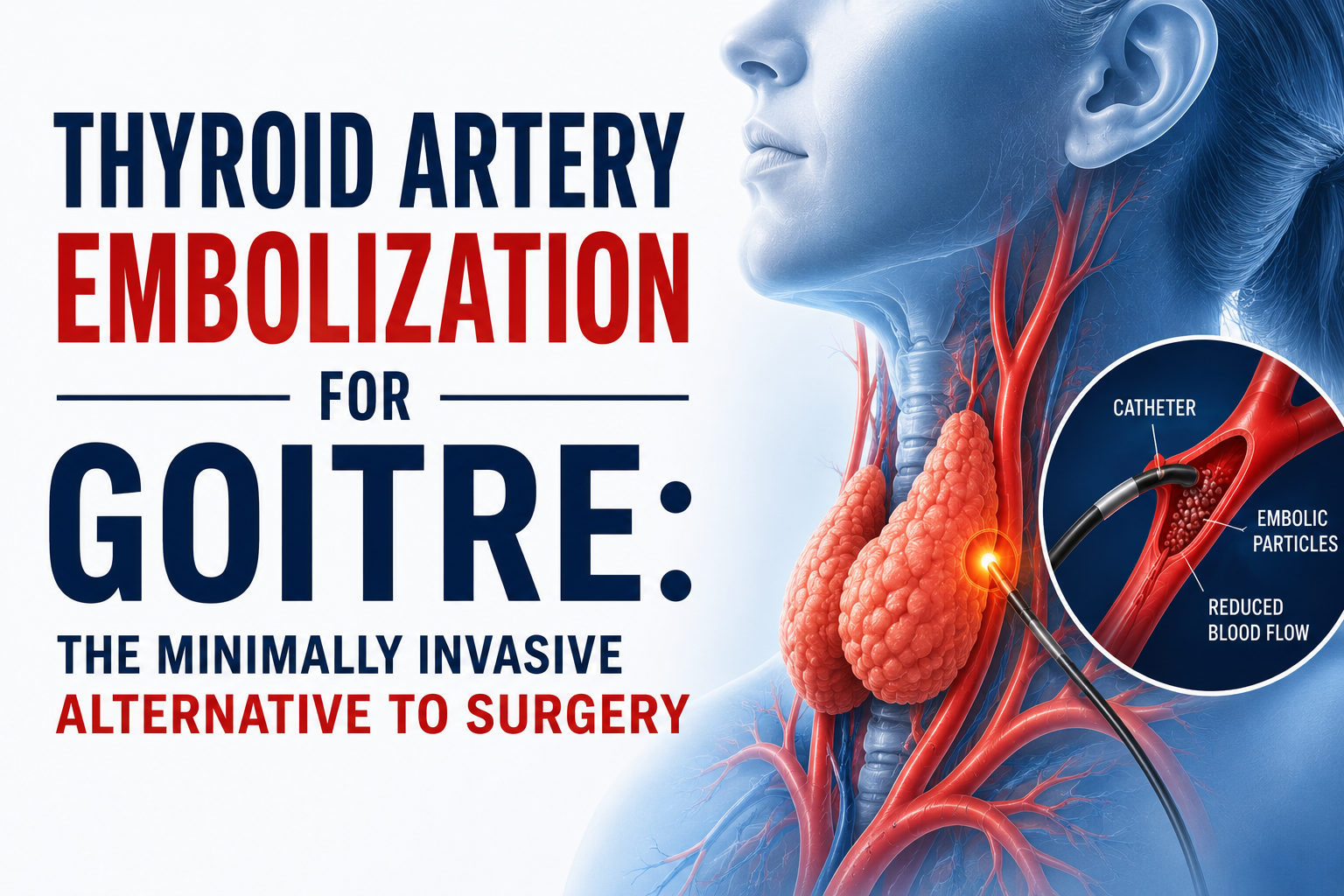
Thyroid Artery Embolization (TAE) is a minimally invasive, image-guided procedure performed by an interventional radiologist to deliberately reduce the blood supply to the thyroid gland, causing it to shrink over the following weeks and months.
The underlying principle is elegantly simple: the thyroid gland like all tissues requires a continuous blood supply to maintain its size. By selectively blocking the arteries that feed the enlarged gland, TAE induces a gradual, controlled reduction in gland volume without the need for any incision, general anesthesia, or hospital stay beyond 24 hours.
The procedure was developed from embolization techniques already well-established in interventional radiology for conditions such as uterine fibroid embolization, prostate artery embolization, and hepatic artery embolization for liver tumors. These techniques have decades of safety data behind them.
How much can TAE shrink a goitre?
Asper researches Thyroid volume reductions of 40–60% within 6–12 months after TAE. Compressive symptoms — including difficulty breathing and swallowing — typically improve significantly within 4–8 weeks. In some patients, a second session can achieve additional volume reduction.
- Who Is a Candidate for Thyroid Artery Embolization?
TAE is not a one-size-fits-all solution, but it is an excellent option for a carefully selected group of patients.
You may be a good candidate if:
- Large benign goitre causing pressure symptoms
- High surgical risk due to age or medical conditions
- Previous neck surgery with higher re-operation risk
- Multinodular or hypervascular goitre
- Toxic multinodular goitre when RAI is unsuitable
- Patients who prefer to avoid surgery
- Patients on blood thinners
- Recurrent goitre after prior treatment
TAE is not recommended for:
- Suspected thyroid cancer
- Small, symptom-free goitres
- Pregnancy
- Severe artery disease preventing safe catheterization
The TAE Procedure: Step by Step
- Pre-procedure Evaluation
Ultrasound, thyroid tests, FNAC, and imaging are done to confirm suitability. Certain medications may be adjusted, and fasting is required before the procedure. - Catheter Access
Under local anesthesia and mild sedation, a small catheter is inserted through the wrist or groin artery and guided to the thyroid arteries. - Angiogram
Contrast dye is used to map the thyroid blood vessels and identify the arteries supplying the goitre. - Embolization
Tiny particles are injected to block blood flow to the enlarged thyroid tissue, causing it to shrink over time. - Recovery
The catheter is removed, and patients are monitored briefly. Most go home within 24 hours with mild temporary discomfort.
Procedure Duration:
Usually takes about 60–120 minutes.
- Benefits of Thyroid Artery Embolization
The advantages of TAE over surgical thyroidectomy are substantial, particularly for patients who are not ideal surgical candidates:
- No general anesthesia required
- No surgical cuts or neck scars
- Thyroid function often preserved
- No risk of voice nerve injury
- No risk to parathyroid glands
- Short hospital stay (same day or overnight)
- Faster recovery within 3–5 days
- Significant goitre shrinkage with symptom relief
- Procedure can be repeated if needed
- Safer option for elderly and high-risk patients
- Potential Risks and Side Effects
TAE is generally safe, and serious complications are rare when performed by an experienced interventional radiologist.
Common Temporary Side Effects
- Mild neck pain or swelling
- Low-grade fever
- Fatigue or nausea
- Temporary inflammation before shrinkage
Less Common Risks
- Temporary thyroid hormone imbalance
- Hypothyroidism requiring medication
- Bruising at the catheter site
- Contrast allergy
Rare Serious Complications
- Non-target embolization
- Skin damage or infection
Safety:
Major complication rates are low (less than 2–3%) and compare favorably with thyroid surgery.
Conclusion
Thyroid Artery Embolization (TAE) offers a safe, minimally invasive alternative to surgery for patients with benign goitre. With faster recovery, no neck scar, and lower surgical risk, it is especially valuable for elderly or high-risk patients.
FAQ’s:
Is Thyroid Artery Embolization painful?
TAE is done under local anesthesia with minimal discomfort. Mild neck pain for 1–3 days may occur and is manageable with medicines.
Will TAE affect thyroid hormone levels?
Most patients maintain normal thyroid function after TAE. Regular monitoring is done, and any hormone imbalance can be easily treated.
How is TAE different from RFA?
RFA treats individual nodules using heat energy, while TAE reduces blood supply to larger or multinodular goitres, making it ideal for diffuse thyroid enlargement.