Radiofrequency Ablation for Osteoid Osteoma
Imagine waking at 2 a.m. every night not from anxiety or noise, but from a deep, drilling ache in your femur, shin, or spine that nothing seems to stop except a handful of ibuprofen tablets. For thousands of young patients across India, this is not a hypothetical. It is everyday life with osteoid osteoma. The good news? There is now a permanent, one-session cure that does not require a single surgical cut.
What Is Osteoid Osteoma?
Osteoid osteoma is a small, benign (non-cancerous) bone-forming tumor technically classified as a benign osteoblastic neoplasm. It is not life-threatening, does not spread to other organs, and does not transform into bone cancer. However, its ability to cause severe, chronic, and often functionally disabling pain makes it a condition that genuinely demands treatment.
The tumor consists of a central, highly vascular core called the nidus (Latin for “nest”), which is typically a tiny round or oval lesion measuring 0.5–1.5 cm surrounded by a zone of reactive sclerotic (hardened) bone. The nidus contains immature bone matrix, blood vessels, and nerve fibers — and it is the nerve fibers and prostaglandin production within this nidus that generate the characteristic, severe pain.
Common Anatomical Locations of Osteoid Osteoma
Osteoid osteoma can develop in any bone, but it commonly affects these areas:
Femur (Thigh Bone)
The most commonly affected site
Tibia (Shin Bone)
One of the frequently affected bones
Spine (Vertebrae)
Especially the posterior elements of the spine
Hand & Wrist
Including carpals, metacarpals, and phalanges
Foot & Ankle
Commonly affects the talus and calcaneum
Humerus (Upper Arm)
Usually seen in the proximal or mid-shaft region
Symptoms of Osteoid Osteoma
Night pain that often wakes patients from sleep
Pain relief with aspirin or NSAIDs
Deep, localized aching pain
Limping or gait changes in leg lesions
Muscle weakness from reduced limb use
Scoliosis or stiffness when the spine is involved
Gradually worsening pain over time
The average time from symptom onset to correct diagnosis of osteoid osteoma is 12–36 months. Many patients are first told they have growing pains, sports injuries, tendinitis, or even arthritis. If you or your child has bone pain that responds dramatically to ibuprofen but returns reliably at night, ask specifically about osteoid osteoma and request a CT scan of the painful area.
Who Gets Osteoid Osteoma?
Most commonly diagnosed in individuals aged 5–25 years, with peak incidence in the teenage years Significantly more frequent in males (approximately 2–3 times more common than in females) Can affect people of all ethnicities and geographic backgrounds Most common in the long bones of the lower limbs (femur and tibia) Rarely diagnosed after age 40, though it does occur Not associated with malignancy — osteoid osteoma never transforms into bone cancer
Who Gets Osteoid Osteoma?
Diagnosis is based on clinical history and imaging studies.
Night pain with dramatic relief from NSAIDs is a classic sign of osteoid osteoma.
CT Scan — the gold standard for identifying the nidus and planning treatment
X-ray — may show surrounding dense bone changes
MRI — helps detect bone inflammation and spinal or joint lesions
Bone Scan — shows a “hot spot” at the affected area
In many cases, a separate biopsy is not needed, as diagnosis and treatment can be performed together during CT-guided RFA.
Traditional Treatment Options & Their Limitations
Long-term NSAID use may temporarily relieve pain, but the lesion remains active and prolonged use can affect the stomach and kidneys.
Open surgery was once the standard treatment but involves hospitalization, surgical risks, longer recovery, and possible recurrence.
CT-Guided Radiofrequency Ablation (RFA) is now the preferred treatment — minimally invasive, highly effective, with faster recovery and minimal downtime.
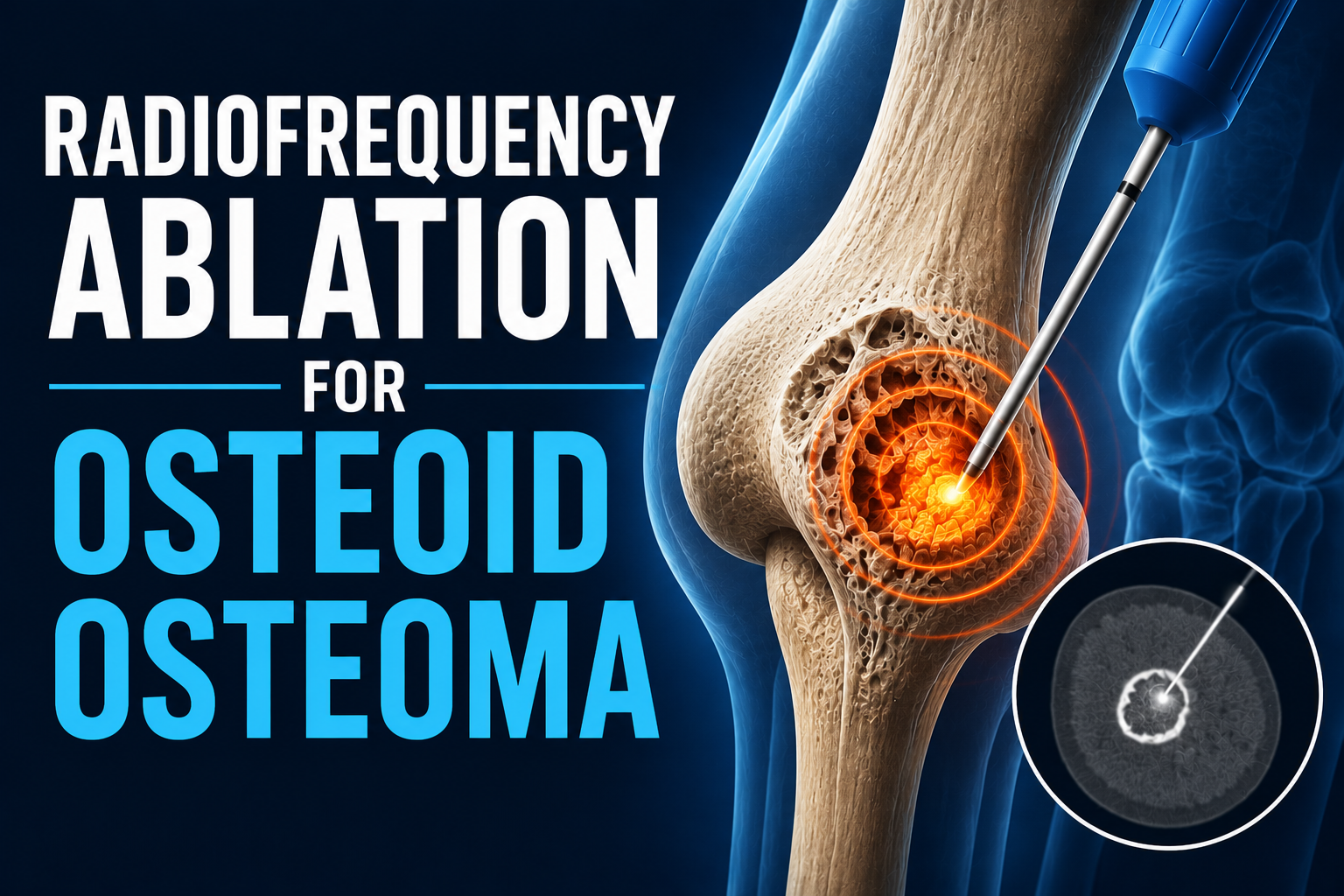
What Is CT-Guided Radiofrequency Ablation (RFA)?
CT-Guided RFA is a minimally invasive treatment for osteoid osteoma that uses heat generated by radiofrequency energy to destroy the painful nidus inside the bone.
CT guidance helps the interventional radiologist precisely place the needle into the tiny lesion with high accuracy.
Heat treatment destroys the pain-producing cells and nerve fibers without damaging the surrounding healthy bone.
The result: effective pain relief, minimal downtime, and faster recovery without major surgery.
Who Is a Candidate for CT-Guided RFA?
CT-guided RFA is appropriate for the vast majority of patients with symptomatic osteoid osteoma. Specifically, excellent candidates include:
Patients with imaging-confirmed osteoid osteoma causing persistent, functionally disabling pain
Patients on long-term NSAIDs who wish to eliminate medication dependence
Children and adolescents where prolonged NSAID use poses developmental and growth concerns
Athletes and active individuals for whom rapid return to sport or activity is a priority
Patients in whom the lesion is not immediately adjacent to critical structures (see below)
Patients with recurrence after previous surgery or ablation (repeat RFA is feasible)
Patients in whom open surgery would be technically difficult (e.g., deep femoral neck, sacral, or spinal lesions)
The CT-Guided RFA Procedure
Pre-procedure planning includes imaging review, blood tests, and preparation before treatment.
The procedure is performed under anesthesia or deep sedation for comfort and precise needle placement.
Using CT guidance, the needle is accurately placed into the tiny nidus inside the bone.
Radiofrequency energy heats and destroys the pain-producing lesion while preserving healthy tissue.
A final CT scan confirms success, and most patients return home the same day with minimal downtime.
Benefits of CT-Guided RFA for Osteoid Osteoma
High success and cure rates with minimally invasive treatment.
Precise CT-guided targeting destroys the nidus while preserving healthy bone.
No major surgery, large incision, or prolonged hospitalization required.
Most patients experience rapid pain relief within 24–48 hours and return quickly to daily activities.
Safe and effective for children, adolescents, and active individuals while reducing long-term dependence on pain medications.
Frequently Asked Question
How long does pain relief take after RFA for osteoid osteoma?
Most patients experience significant pain relief within 24–48 hours after the procedure, with many becoming pain-free within the first week.
Is osteoid osteoma cancer? Can it spread?
No. Osteoid osteoma is a completely benign bone tumor. It does not spread to other parts of the body and never turns into bone cancer. The main concern is the pain and discomfort it causes, which can be effectively treated.
Can osteoid osteoma recur after RFA?
True recurrence after successful RFA is very rare. In most cases, persistent symptoms occur due to incomplete initial ablation rather than regrowth of the lesion. Precise CT-guided targeting is the key to successful treatment.
Conclusion:
Osteoid osteoma may be small, but the pain it causes can greatly affect daily life and sleep. Fortunately, CT-guided Radiofrequency Ablation (RFA) offers a highly effective, minimally invasive treatment with rapid pain relief and faster recovery compared to surgery.
If persistent night bone pain responds to painkillers like ibuprofen, early evaluation and expert consultation with best interventional radiologist in hyderabad Dr. Suresh Giragani can help achieve a quick and lasting cure.